



This colony is often termed as the end-of-the-road area – isolated and exiled from rest of the world.
By Muntaha Mehraj Hafiz
A cleric’s voice heralds dawn at a sickbay sheltering stigmatised souls of the valley. In this Srinagar sanatorium nestled at a placid upland overlooking a misty lake, a meditative morning is driving out the silence of social seclusion.
Young boys and girls recite Quranic verses in a unanimous tone inside a single-room seminary. Sanctified texts, worn-out carpets and muddy walls make it a specious spiritual shelter for the young children – the third generation of Leprosy patients, of Baharaar: the only, and probably the last leprosy hospital in Kashmir.
At the seminary’s roughly-painted door, Ayesha is cooling her heels. The 28-year-old is a mother of three kids, but she’s worried about her daughter’s learning ability.
The young one is showing no signs of improvement despite it being her second year in seminary. Last time, she was bullied at the school and since then she requires regular prompting in her learning engagement.
“After that incident,” says Ayesha, concerned about her six-year-old’s mental health, “my daughter has been reluctant about school. She has been asking me questions about leprosy. And I tell her it’s nothing to worry about.”
A place like Baharaar faces a 130-year-old trajectory of discrimination and stigma from the outer world. But while men have learned to cope with the external pressures, the women and children lack behind.
Like most of the challenges in the world, fighting prejudice against leprosy patients, survivors and their families has been a matter of concern.
According to the latest figures provided to World Health Organization (WHO) by 139 countries, 127558 new leprosy cases were detected globally in 2020, showing a decline of 37 to 50 per cent.
In India, the country with the highest number of cases, the rate of visible deformities is 1.1 per million population.
Back in the day when the same ailment spread its tentacles in the valley, Baharaar was situated in Srinagar by the Imperial British in 1894 under the “Kashmir Medical Mission”.
Over a century later, the route towards the colony opens in a wide road twinning with beauty and grief. The right side has the sparkle and freshness of a jewel-like eutrophic lake marked by willow and poplar trees, while the left end has two graveyards dotted with around 300 graves of the past generations of the residents.
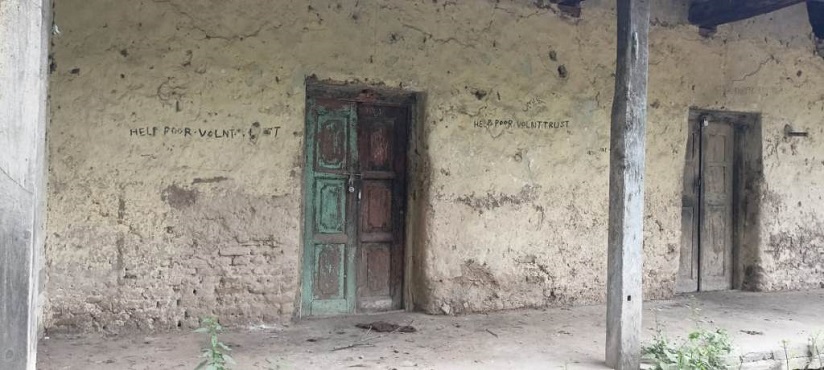
This colony is often termed as the end-of-the-road area – isolated and exiled from rest of the world.
Built over an expanse of 39 acres – the hospital-turned-home has 64 residential apartments accommodating more than 250 people –young, old and children including 70 patients who survived Leprosy.
The new quarters with two rooms and an attached washroom lie adjacent to old billets and are the windowless mud huts with high ceilings.
These structures wouldn’t allow a speck of light to enter, alike to a mausoleum. And in the middle of the colony is a huge deck built around the 500-year-old Chinar tree where men and women often sit to discuss their daily affairs.
Exiled From Homes

62-year-old Noora sits on the porch of her two-room apartment. With glint in her eyes, she likes to have a view of children playing in the narrow pathways of the leprosy colony. Her demeanour looks sturdy but a shade of exhaustion is evident on her face. Her story of Leprosy begins when she was a 14-year-old.
“I was playing with my friends, and suddenly I felt numbness in my right hand,” Noora recalls her day of doom. “For days, I overlooked it but it eventually spread to my whole arm. In a state of fear my father rushed me to a district hospital and doctors after a short deliberation diagnosed me with leprosy.”
Hailing from south Kashmir’s Kulgam district, Noora lived in a joint family of 14. Being the youngest child among her six siblings, she was the pampered one.
However, as the news of her disease broke amongst her relatives, the scenario changed. She clearly remembers how her father was pressurized to expel her from the house, and how he beseeched his brothers to let his daughter live there in a separate room.
“This disease was considered a curse,” recounts Noora in a difficult tone. “Everyone treated me like I was a bad omen.”
The family fuss ended one fine morning when Noora’s father wrapped a blanket over her and silently left for Baharaar.
As a girl of a tender age, Noora barely understood why she was treated so miserably. She was cold. However, she knew she was an outcast.
Noora’s new home—Baharaar—was allocated on the immediate orders of the then commander in chief of India, Lord Roberts during the inception of leprosy in Kashmir during 19th century.
Initially, the hospital admitted 25 patients and as cases of leprosy escalated, the number increased. During 1970s, when Noora arrived, around 150 patients were admitted in the hospital – men and women, from various parts of the erstwhile state of Jammu and Kashmir.
“When my father brought me here, I wept for a month,” Noora continues to narrate her life trauma. “Everything seemed lifeless. The walls of my quarters haunted me and I wanted to return home. But when I met patients with the severe cases of leprosy, I stopped complaining and learnt to live with it.”
Among all the patients, Noora remembers Ali Muhammad who was the oldest and among the first 40 patients admitted to the hospital. Ali was a 90-year-old cleric, who tied her knot with one Mohammad Sultan.
Like her other inmates in the colony, Noora began a new chapter of her life, and Baharaar turned into a place of suffering and ease, sorrow and happiness, longing and relief.
A decade after this, in 1980, a sigh of relief descended as MDT—Multidrug therapy—was discovered, and leprosy became a treatable disease. Eventually, as the disease was contained at Baharaar, no new patient was admitted after the year 2000. However, for patients like Noora, the battle for a better identity is still ongoing.
“The stigma has been worse than the disease,” says Noora as she pushes her knees to gear back to her routine work. “Leprosy left us crippled but the society left us exhausted.”
Deformities: Visible and Hidden

It’s not uncommon how women with leprosy are more vulnerable to discrimination when compared to their male counterparts primarily due to their gender and then due to the disabilities that result from the disease.
Women living at Baharaar consider themselves untouchables and outcasts due to their disability. Most of them have deformed limbs, and blind eyes. Abandoned by their loved ones, this has impacted their self-confidence, mental health and economic self-sufficiency.
“We no longer feel like humans,” says Maqsooda, picking collard greens from her kitchen garden. “This is a living death.”
She clutches the basket by her arm and moves towards her quarter. She uses her fists to open the door, and rests on the chair to catch her breath. Both of her hands and feet are crippled due to nerve damage caused by leprosy.
Leprosy is a chronic infectious disease caused by a bacillus, Mycobacterium leprae. It multiplies slowly and the incubation period of the disease is 5 years.
Symptoms of the disease may occur within 1 year but can also take as long as 20 years to develop. Leprosy mainly affects the skin, the peripheral nerves, mucosa of the upper respiratory tract, and the eyes.
A team of dermatologists, pathologists work closely to detect leprosy.
“More commonly leprosy starts with an anesthetic patch on the body and this patch can be seen over the abdomen trunk, buttocks, legs with either fewer or no sensations at all,” says Dr Umar, Dermatologist, GMC Anantnag. “This is mainly a dry patch on the body which leads to nerve enlargement of the peripheral nerves of the body.”
If the peripheral nerves are found to be enlarged in the patient, and a dry patch is found, the medico says, it’s suggestive of leprosy which is further confirmed by performing a slit-skin smear test on the patients.
Maqsooda too was diagnosed with a reddish white patch on her skin but until she would know about the disease the bacterial infection initiated chronic non-healing ulcers on her feet and hands.
At this moment, she was a 26-year-old. And soon, she was admitted to Baharaar by her brother who never returned to meet her again. She’s married to a fellow patient and has two children now.
“My mother wanted to come with me,” says Maqsooda, rubbing sweat with her pink dupatta shading her crippled hand. “But my family didn’t allow her. What can be worse than your own family disowning you?”
As Maqsooda reaches out to get her medicines for osteoarthritis from the two-toned almirah besides her, she wishes to be as efficient as other women. But at the same time, she feels disheartened due to her destiny: “Myani khoth khaste kus chu? Ye daghh cha anaan waelith” (Who’s worse than me? This pain consumes you and kills you slowly).
The stigma and fear associated with transmission of the disease is so ingrained that women at Baharaar don’t move out of their colonies, until it’s an emergency. Some patients prefer to stay indoors, even if there’s a serious health condition. One such case is of Saira Rafiq.
Until last week, the 47-year-old woman took medications without consulting a specialist but when in the middle of the night she had difficulty in breathing, she was rushed to SKIMS in the stationed ambulance at the colony that ferries patients when required. She was diagnosed with Pneumonia.
Saira’s encounter with the outside world has been unfortunate. Leprosy has disfigured her face. With a flattened nasal cavity, thickened skin of forehead and chin, and with multiple nodular lesions all over her face, she has been covering her facial deformity since last 10 years.
“I don’t like to go out in public,” says Saira in a hoarse voice. Due to her persistent dry cough she pauses for a moment, to speak again. She has been fearful after someone at a local health centre had called her a demon.
“People fret over our presence,” she continues. “There’s no social participation for people like us. Not only people but doctors also look down upon us.”
She lays open all her documents to reveal her worsening health condition. Besides leprosy, she’s been treated for hypertension, thyroid and herniated discs.
The medical officer had suggested her to visit a physiotherapist for her neck pain, but the dearth of trained physiotherapists for Leprosy patients in Kashmir has made the situation even more challenging.
“Physiotherapy plays an important role in treating leprosy patients,” says Dr Arif Ahmad, one of the senior physiotherapists from Srinagar’s SMHS Hospital.
“We identify the nerve function impairment at the earliest, and keeping in view the condition of the patient, indulge in pre- and post-operative rehabilitation process that prevents further deterioration of limbs.”
As experts, Dr Arif continues, physiotherapists also focus on imparting education on lifestyle modification skills and self-care techniques to the patients which help improve the emotional, psychological and physical state of the patient.
“But many physiotherapists in Kashmir lack expertise in leprosy and disability,” the medico says. “We require partnership with state and central government so trainings and workshops are conducted in Kashmir. This is essential.”
Patients like Saira suffer in silence. For now, she cannot contemplate going to a physiotherapist as she’s worried about ‘other’ medical expenses that her family cannot afford.
“Where shall I get money for such costly MRI’s and blood tests? We all here are helpless,” complains Saira.
Although under the supervision of directorate of health services, a medical centre for “basic” health check-ups is functional in the leprosy hospital but it is devoid of para-medical services and as of now is one of the “major concerns” of the under-privileged inhabitants at Baharaar.
Battling Lifetime Seclusion
While some women were segregated by their immediate families, many faced cruelty and abuse at the hands of their husbands after being diagnosed with leprosy, ending their marriages miserably.
As one steps inside the leper colony, an aura of gloom and solitude descends. But what if there’s solitude within solitude, isolation within isolation? Many patients found love, care within the community, and raised families except a few who’re still living a life of loneliness, pain and struggle, like Khatija.
She migrated from Ladakh to Srinagar in 1992 with a fellow inmate. Her story of leprosy is almost identical to other women at Baharaar: clawed hands, disfigured face, suppurating sores oozing pus and blood. But she’s blind too. And what makes her struggle extraordinary is: her devotion to fight leprosy – all on her own.
More than the disease, it was her husband’s cold behaviour toward her that caused her relentless agony. She was 32-year-old when she arrived at Baharaar. Her disease initiated with a dry patch on her arms that made her husband suspicious of her disease and out of fear, one day he dragged her out of the house.
“Instead of taking me to a doctor my husband thrashed me,” says Khatija in a mix of two languages, Balti –her native language, and Kashmiri, that she picked in the colony.
“I was an orphan. Where would I go? Moreover I was pregnant with his child. He didn’t even consider that.”
Khatija lived with her aunt until she delivered a baby. After which, she left for Baharaar. That year her husband had married another woman.
Khatija’s appearance is lean, and her entire body is reduced to a body of a small child. For a 62-year-old, the condition is pitiful. Her bulging white eyes have lost the radiance and her struggle is real.
“No other affliction causes as much pain and agony as leprosy. My husband took my son away and never visited me,” says Khatija. “Nor did my son,” she whispers timidly.
Khatija barely cries but when her eyes go dry a tear falls down. It’s the modulation of her voice that signals how lonely she feels. She’s been taken care by her neighbours who come and cook for her. For her nurturing, she submits her stipend to them. “What would I do with the money,” she says. Surprisingly, where family left them to die, strangers extended a helping hand to them.
At present, the Directorate of Health Services Kashmir provides food, supportive medicine and clothes to the patients at Baharaar. They also receive a monthly allowance of Rs.1000 by the Department of Social Welfare which they feel is “not enough.”
Khatija’s son is terrified to meet his own mother, as communicated to her via some relative. She shrinks her body, as she expresses her last wish: “I want to talk to my son. He can see me through the window if he fears to meet me here. I’ll not touch him,” says Khatija. “A child can hate his mother but a mother cannot hate her child even if he creates a mountain of troubles for her.”
Stigma associated with leprosy has rendered patients helpless. Some are attended by fellow inmates while some live in isolation, all alone in a terrible mess.
At one of the shrines located 2 kilometres away from the Leprosy Colony, a group of women raise their hands to pray as head priest displays holy relic to the devotees. In a huddle of women, a visually impaired lady stands quietly at the back of the row. Following her intuition, she prays in the direction of other women.
She’s Zeba, a 78-year-old inhabitant of Kupwara—now a patient at Baharaar.
She visits the shrine once a year – on the eve of birth anniversary of Prophet Muhammad. With her apparent disability, she has oriented herself to adjust in a group of people who at first saw her as a threat.
“At times women sit away from me. And I don’t mind that,” says Zeba who has been fighting the disgrace and distinction for 40 years now.
When she was diagnosed with leprosy she was banished from her village, and forced to live in separation from her husband, along with her 2-year-old son.
Due to lack of knowledge, and awareness among the community members, many believe leprosy is highly contagious, which has led to ostracization and discrimination of patients.
“Leprosy is a communicable disease but one cannot get leprosy by shaking hands, casual social contact, sharing food or by sitting with the affected people,” says Dr Aliya, Pathologist SKIMS.
“Leprosy,” the medic explains, “is likely transmitted when there is a prolonged close contact with someone with untreated leprosy, or when a person coughs or sneezes and the germ enters the body of a healthy person via droplets containing bacteria.”
Presently, if a person is diagnosed with leprosy he’s cured within a year of transmission. In 1981, WHO recommended MDT for the treatment of leprosy. Currently, it has recommended MDT which consists of medicines: Dapsone, Rifampicin, and Clofazimine.
This treatment is prescribed for 6 months to patients with Paucibacillary leprosy (PB), and 12 months for Multibacillary (MB) cases. MDT kills the bacteria and the patient is cured.
As the head cleric at the shrine finishes the prayer, Zeba folds her prayer mat, adjusts her black sunglasses that protect her against light sensitivity and bends down to lift a wooden stick that helps her navigate back towards the colony.
Leprosy has invaded her facial nerves, resulting in acute corneal ulcers in her eyes. She has no vision in her left eye and failing eyesight in her right.
Zeba’s son works as a daily-wager, and returns home at midnight. Until then, with her stubby hands, bleeding numb feet and blindness, she manages to cook and clean.
At her allotted room at Baharaar, the hygiene is missing. There are heaps of garbage lying at the door, with dust-ridden carpets, and worn-out beddings, she sits at a corner of this dilapidated space. But when guests visit her, she never fails to offer a clean carpet to them.
Zeba is surviving through tough times but this is evident that blind patients at Baharaar are the worst sufferers. This negligence questions the contribution of government towards the well-being of leprosy patients and also, the supervising department that vows to provide quality life to this marginalized group.
Concern For Future Generations

More than 16 million leprosy patients have been treated over past 20 years, and a general reduction in new cases has been observed in several countries. However, discrimination against the patients and their families doesn’t cease to exist.
People diagnosed with leprosy are ripped off their basic fundamental rights such as right to equality, right to education and right to all opportunities in matters of employment, marriage and health.
“We are not considered part of the society,” says Yasmin, a 28-year-old resident of Baharaar. “We are living a life of untouchables. Nobody wants to understand that our families are no longer contagious.”
Yasmin was 4-year-old when her mother was diagnosed with leprosy. Since then, a track of “disgrace” and “misery” has been following her, persistently.
It’s been 12 years since her mother has been cured of leprosy, but the family is suffering—psychologically and emotionally.
Contemplating Yasmin’s marriage for 3 years now, they’ve failed to find a better match for her.
“Women living at leprosy colonies often struggle to find better families for themselves,” says Yasmin. “Even my brother was rejected by many families for the same reason. Consequently, we had to get him married to a non-local girl.”
This is not the only case. There are dozens of other women who’re struggling and they either end up marrying someone from the countryside or within the community, often against their will to do so.
Another challenge for young girls and women at Baharaar is lack of opportunities in terms of job and education. Many drop out of school while struggling with bullying, low self-esteem, poor academic performance, and poverty.
“I want to continue my studies but who will pay my school expenses?” says Rufaida, keenly embroidering a shawl, that’s spread over her knees.
Rufaida passed her Class 10 in 2018. Now she’s employed at a small manufacturing unit that sells shawls and stoles. Apart from the stipend that her family receives from the government, she earns Rs 3000 a month. At such a tender age, Rufaida has assumed both domestic as well as economic responsibilities of her family but sadly, at the cost of her dreams.

In pursuit of a better future and life, a few residents have moved out from Baharaar. But the majority—with their children and grandchildren—stay back.
Despite being the third generation of treated leprosy patients, there are individuals who lie or hide about their predecessors, out of fear of inequity, and backtalk.
Nusrat Ara belongs to third-generation of Leprosy patients. She has lately completed her post-graduation and joined a private school. However, she has not disclosed her “real address”, to her colleagues.
“I don’t feel comfortable telling them that I reside at Baharaar,” says Nusrat. “I did that once at a hospital, and the doctor denied treating my ailing father.”
Due to stigma associated with the disease, descendants of leprosy patients often shy away from attending any social gathering. Reminiscing the struggle, and trials of growing up in a leprosy colony, Nusrat says: “We are straddling between two worlds. What future do we have? How many times do you find someone from the colony buying provisions or travelling freely like everyone else? This is because we don’t have policies that would facilitate our inclusion and participation in the society.”
Despite several challenges, the community exhibits such love and brotherhood that binds them together, in any worse or privileged situation.
Among the younger generations of leprosy patients, a lady has set an example. She’s Najma, a 65-year old who lives at the outskirts of the colony. Her husband purchased the land in the vicinity so she can live close to the place where her parents lived.
Najma rewinds her memory back to 1960’s when 350 patients were admitted to the hospital. “I have witnessed a sea of affliction, and tragedy here,” she recalls. “People who belonged to affluent families saw themselves diminishing.”
Najma was the only daughter of her parents. She was a keen child, and her analysis of pain turned her into a spiritual figure. Now she assists women at Baharaar in matters of Islamic jurisprudence, and helps them unburden their melancholy-filled hearts.
“At this age, they feel lonely and helpless, and all they need is a listening ear,” reflects Najma.
Leprosy patients often visit Najma to either have a chat, or get their clothes stitched and hair combed. For the place that nobody wants to visit, and bodies no one wants to touch, she’s an official mortician for the women of the community.
“They don’t have a female attendant here. And it’s difficult to wash the body of a leprosy patient,” says Najma. “Due to pain and suffering, their bodies are in a miserable condition, so one has to be careful. You have to turn and wash their bodies like a flower. I will do that as long as I have the strength to do so. Death is for each one of us—and that’s what we should never forget.”
Follow this link to join our WhatsApp group: Join Now
Be Part of Quality Journalism |
Quality journalism takes a lot of time, money and hard work to produce and despite all the hardships we still do it. Our reporters and editors are working overtime in Kashmir and beyond to cover what you care about, break big stories, and expose injustices that can change lives. Today more people are reading Kashmir Observer than ever, but only a handful are paying while advertising revenues are falling fast. |
| ACT NOW |
| MONTHLY | Rs 100 |  |
| YEARLY | Rs 1000 | |
| LIFETIME | Rs 10000 | |








